
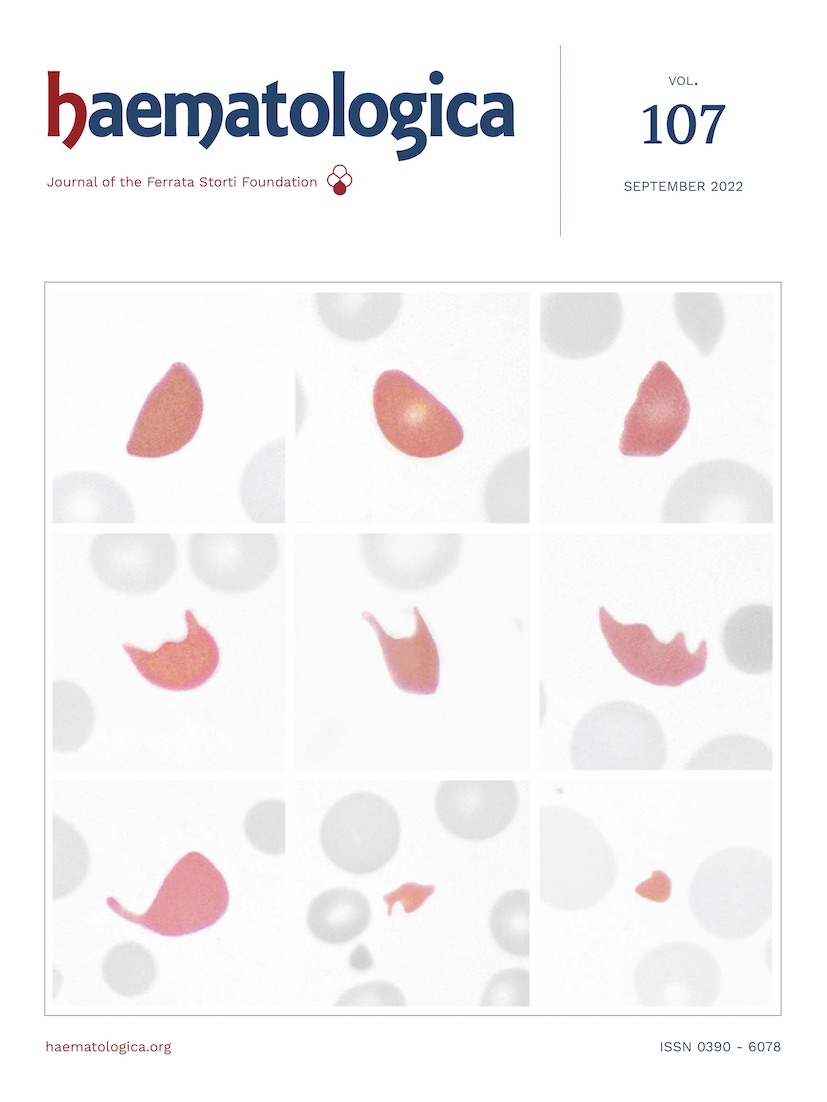
The presence of schistocytes is a constant feature of patients with thrombotic microangiopathies. The highest concentrations of schistocytes are observed in thrombotic thrombocytopenic purpura in which they represent 1-18% of red blood cells. Lower concentrations can be observed in other thrombotic microangiopathies as well as in subjects with mechanical heart valves or other intravascular devices and in chronic renal diseases. Helmet cells (A-C, arrow) are erythrocytes with an amputated zone highlighted by a straight border as a result of a crash on a fibrin strand. The missing cell portion corresponds to the fragments of erythrocytes shown in (H) and (I). Keratocytes (cells with horns) (D-F, arrows) are characterized by two or three spicules separated by concave segments of membrane and have been formed by rupture of peripheral pseudovacuoles and subsequent fusion of the cell membrane. Fragments of erythrocytes with bizarre shapes escape a precise classification (G-I). In (F) and (G) you can also recognize microspherocytes, which are a secondary manifestation of fragmentation and should be included within the schistocyte count only in the presence of the shape abnormalities described in (A-F).1
Footnotes
Correspondence
Disclosures
No conflicts of interest to disclose.
References
- Balduini CL. Thrombotic microangiopathies. Haematologica. 2020; 105(Suppl 1):270-275. https://doi.org/10.3324/haematol.2019.244939PubMedPubMed CentralGoogle Scholar
Figures & Tables
Article Information

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.