
Abstract
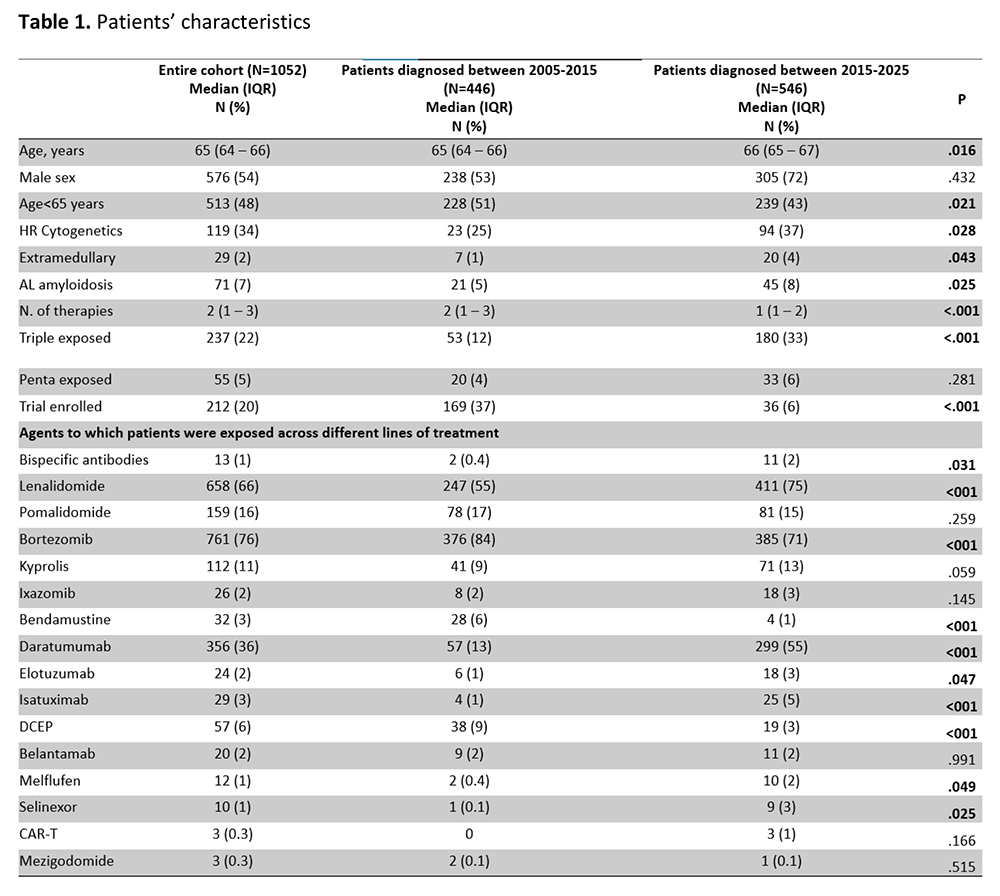
Therapeutic innovation in multiple myeloma (MM), through the sequential integration of immunomodulatory drugs, proteasome inhibitors, monoclonal antibodies, cellular therapies, and bispecific antibodies, has significantly improved survival outcomes. Alongside novel agents and combinations, optimized supportive care strategies have reduced treatment-related toxicity and improved disease control. However, traditional efficacy endpoints may not fully capture the real-world benefit of these advances. In this context, attrition rate (AR)—defined as the proportion of patients who die without receiving the subsequent line of therapy (LOT) after progression—represents a clinically meaningful indicator of treatment feasibility, disease aggressiveness, and patient vulnerability across the MM disease course. We retrospectively analyzed clinical characteristics and treatment patterns of 1052 patients diagnosed and treated for MM at our Institution between January 2005 and September 2025. Most patients were managed in a real-world setting outside clinical trials. Patients were stratified according to therapeutic era: Group A, diagnosed between 2005 and 2015 (n=446), and Group B, diagnosed between 2016 and 2025 (n=546). Patient characteristics are summarized in Table 1. After a median follow-up of 107 months (95% CI: 98–243), the median overall survival (OS) for the entire cohort was 65 months (95% CI: 58–69). Treatment strategies evolved substantially over time. Until 2015, patients received a median of 2 LOTs (range 1–10), whereas between 2015 and 2025 the median number of LOTs was 1 (range 1–12). In group A, bortezomib-based chemotherapy remained the predominant first-line regimen (52%). In contrast, treatment patterns in Group B shifted toward anti-CD38–based therapies (36%), including 114 (21%) patients treated in combination with bortezomib and 85 (15%) in combination with lenalidomide. Moreover, repeated use of backbone agents across multiple lines of therapy was more common in group A. In this group, 130 (29%) patients received bortezomib and 61 (13%) received lenalidomide in more than one treatment line, compared with 45 (8%) and 30 (5%) patients, respectively, in group B. AR was defined as the proportion of patients who died without receiving the subsequent LOT after progression. All patients received first-line therapy. AR increased with successive lines of therapy in both groups but declined across therapeutic eras. Overall, AR decreased from 27–42% in group A to 10–31% in group B. Conversely, overall response rates improved overtime in group A, from 3% to 5% but decreased from 48% to 21% in group B, probably reflecting early use of monoclonal antibodies. Specifically, in the 2005–2015 period, AR was 27% after first-line therapy, 37% after second-line, and 33% and 42% after third and fourth lines, respectively. In the 2015–2025 period, corresponding ARs declined to 10%, 20%, 28%, and 31%. In conclusion, despite major therapeutic advances and improvements in supportive care, treatment attrition remains a relevant challenge throughout the MM disease course. Further strategies aimed at optimizing treatment sequencing and maintaining patients on therapy are needed to further reduce attrition rates.
Footnotes
Disclosures
No Conflict of interest.
Funding
No funding.
Figures & Tables
Article Information

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.