
Abstract
Background. Due to the greater awareness of rare diseases that are related to a even small amount of M-protein, the number of patient referrals for M-protein analysis to the hematology outpatient clinic of hospitals in the Netherlands has increased. In order to analyze all these patients in a proper way, a medical care pathway was developed that is initially intensive, but later reduces care by discharging patients with a low-risk MGUS from further monitoring. In this care pathway an extensive and standardized medical history is taken combined with laboratory analysis, including NT-proBNP and urine analysis.
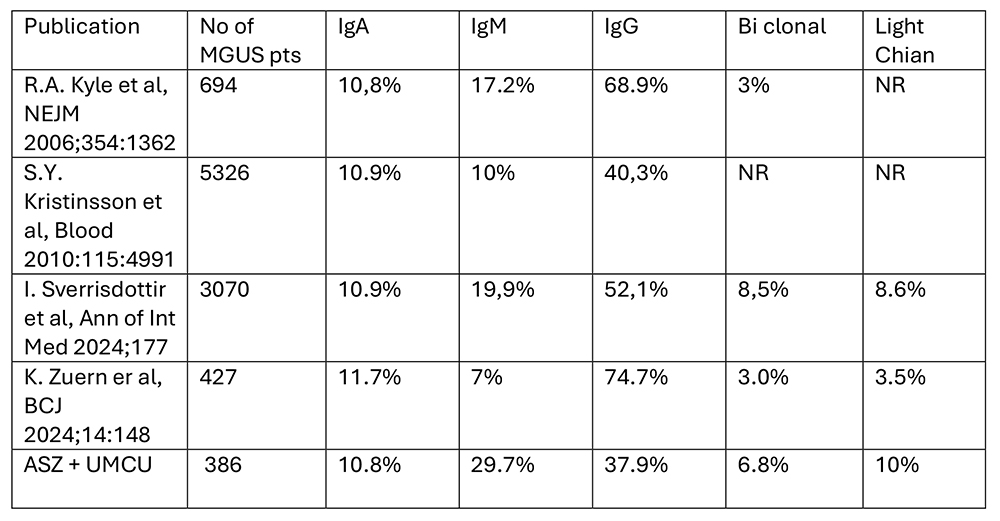
Methods. We analyzed the data from 2 hospitals, one large non-academic hospital Albert Schweitzer (ASZ) and one academic center UMC Utrecht (UMCU). The UMCU is one of the expertise centers for amyloidosis and for neuromuscular diseases in the Netherlands and also a cardiac transplant center. From April 2021 to August 2025, 386 consecutive patients were analyzed and have complete data sets, 117 from ASZ and 269 from UMCU. For the total group, the median age was 69 years, range 30-91, and patients in the UMCU were median 5.5 years younger. Majority of patients were male (63.2%). In both hospitals, most of the referrals were from the neurologists, 32.5% and 39.0%, for ASZ and UMCU respectively. This is probably due to a neurology-based national guideline for polyneuropathy (PNP) that stipulates that in the diagnostic part of PNP analysis, testing for a M-protein is advised. In the ASZ 23.9% of patients were referred by the general practitioner and third largest referrals were from internal medicine (9.4%). In contrast, in the UMCU the cardiology was the second largest group of referrals (11.9%), followed by immunology/rheumatology department with 10.8% of referrals. On clinical indication a decision for further diagnostics is made. Bone marrow examination was conducted in 27,4 and 53.1% of the patients respectively, and also the performance of fat pad biopsies was numerically different between the 2 hospitals, 2.6% in ASZ and 32.0% in UMCU. Radiology was done in 83.8% and 36.4% of the patients in the ASZ and UMCU, respectively. In the ASZ, 4 out of 117 (3.4%) screened patients were diagnosed with a malignancy; multiple myeloma (MM) in 1 and asymptomatic MM in 3 patients. For MGUS related diseases one patient with anti MAG PNP was diagnosed. In the UMCU 8.6% of the patients had a malignancy; AL amyloidosis in 8, Waldenstrom’s macroglobulinemia in 4, asymptomatic MM in 10, and POEMS in 1 patient. MGUS related diseases were found in 8 (3.0%) patients; 1 cold agglutinin disease, 1 Schnitzler syndrome, 2 cryoglobulinemia, 1 anti MAG PNP, 2 SLONM and 1 Castleman’s disease. In total 88.9% and 84.4% of patients were diagnosed with MGUS, 27,9 and 29.5% being IgM MGUS respectively. Compared to literature we found a higher amount of patients with an IgM MGUS in both hospitals. In a small portion of patients no hematological diagnosis was made, sometimes due to transient M proteins.
Results. According to MAYO criteria 32,5% and 48% of patients were low and low intermediate risk and 18.9% and 0.6% of patients high intermediate and high risk.
Conclusions. This analysis demonstrates, probably due to different a priori change or due to different use of diagnostic tools, that the detection of a hematological malignancy and MGUS related disease is different between hospitals: 4,3% in the ASZ and 11.5% in the UMCU. For both hospitals more patients with IgM MGUS are reported compared to literature. Remarkably, 40.5% of patients with an IgM M protein are being referred by neurology, but without a clear increase in diagnosis of IgM MGUS neurological related diseases.

Footnotes
Disclosures
No Conflict of interest.
Funding
No funding.
Figures & Tables
Article Information

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.