
Abstract
Introduction. Measurable residual disease (MRD) negativity is the strongest single predictor of long-term remission in multiple myeloma (MM). Both next-generation sequencing (NGS; FDA-approved in the US) and next-generation flow (NGF) are standard techniques suggested by the IMWG guidelines for monitoring MRD in MM. In the randomized, phase III IsKia trial, a pre-planned, prospective comparison of NGF and NGS was conducted to assess their concordance.
Methods. Patients (pts) received isatuximab-carfilzomib-lenalidomide-dexamethasone (IsaKRd) induction, HDM-ASCT, consolidation and light consolidation vs the same treatment without isatuximab. MRD was assessed by NGF and NGS after induction, ASCT, consolidation and light consolidation in all pts achieving at least a very good partial response (≥VGPR). Samples were centralized in Torino (IT) and Rotterdam (NL) laboratories. NGS was performed by clonoSEQ® (Adaptive Biotechnologies, Seattle, US-WA) and was prioritized, as MRD negativity by NGS was the trial primary endpoint. NGF was performed by IT and NL following EuroFlow standardized protocols. Concordance between NGF and NGS was evaluated quantitatively – using positive cells per million in paired samples at the same sensitivity – and qualitatively (negative vs positive) by calculating concordant over total samples. Cohen's κ coefficient (κ) was used to evaluate the strength of concordance.
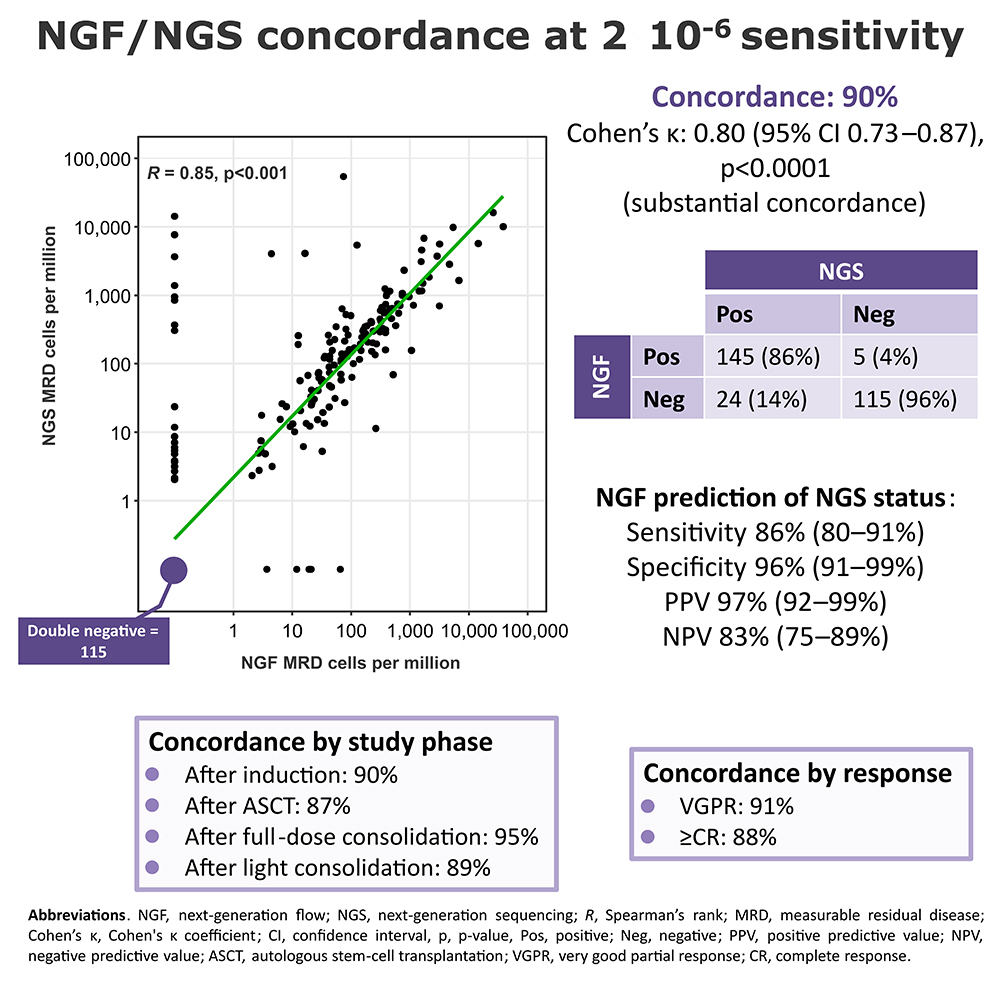
Results. After a median follow-up of 35 months (IQR 32–38), 843 bone marrow (BM) samples were analyzed by NGF. A median number of 6.95 million (IQR 3.51–10) total nucleated cells were analyzed with a median limit of detection of 0.0003% (IQR 0.0002%–0.0006%) per sample. In the ITT population, the MRD negativity rates detected by NGF after each time point were superimposable to those detected by NGS. 692/843 (82%) samples were evaluable at the 10-5 sensitivity by both NGF and NGS. At 10-5, concordance was 89% (κ 0.70). A regression analysis showed a strong positive correlation (Spearman’s rank [R] 0.76; p<0.0001). Using NGS as standard, NGF predicted NGS MRD status with sensitivity of 65%, specificity of 98%, positive predictive value (PPV) of 94% and negative (N)PV of 88%. Since NGS was prioritized, the maximum sensitivity by NGF (2*10-6) was reached in 319/843 (38%) samples, among which 289/319 (91%) were evaluable at the maximum sensitivity of both techniques (2*10-6 by NGF; 10-6 by NGS). At the maximum sensitivity of both techniques, concordance was 88% (κ 0.75). A regression analysis showed a R of 0.85 (p<0.0001). NGF predicted NGS MRD status with sensitivity of 82%, specificity of 96%, PPV of 97% and NPV of 78%. Analyzing both NGF and NGS at a sensitivity of 2x10-6, concordance was 90% (κ 0.80; Figure). NGF predicted NGS MRD status with sensitivity of 86%, specificity of 96%, PPV of 97% and NPV of 83%. No differences were observed grouping samples by clinical phase (after induction, ASCT, full-dose consolidation, light consolidation), conventional response (VGPR vs ≥complete response [CR]) or exposure to anti-CD38 mAbs (IsaKRd vs KRd).
Conclusion. NGF and NGS showed highly concordant results (up to 90% at 2x10-6), suggesting that both may be used to evaluate MRD in the BM in clinical practice. NGF performance was not affected by clinical phase, conventional response or pt exposure to anti-CD38 mAbs. A higher performance of NGF in predicting NGS status was found when a 2x10-6 sensitivity was reached with NGF.

Footnotes
Disclosures
No Conflict of interest.
Funding
No funding.
Figures & Tables
Article Information

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.