
Abstract
Background. Daratumumab-bortezomib-melphalan-prednisone (DVMP) and daratumumab-lenalidomide-dexamethasone (DRd) are standard treatments for transplant-ineligible (NTE) newly diagnosed multiple myeloma (NDMM) patients (pts). No prospective randomized trial has directly compared DVMP vs. DRd. Moreover, real-life older NTE pts are underrepresented in clinical trials.
Aims. We conducted a randomized multicenter phase IV trial (NCT03829371; funded by the Italian Medicines Agency AIFA - Independent Research) to compare safety and efficacy of VMP +/- daratumumab (DVMP) vs Rd +/- daratumumab (DRd) in an unselected real-life population of NTE NDMM pts.
Methods. In the first part of the trial, NDMM pts who were NTE due to age ≥65 years or comorbidities were randomized 1:1 to 9 VMP cycles vs continuous Rd (standard approved schedule). As of July 2022, the protocol was amended to randomize 1:1 pts to DVMP vs DRd. Pts were enrolled regardless of performance status, comorbidities, renal function or baseline laboratory values. Stratification was based on IMWG frailty score and cytogenetic risk [high risk: del(17p), t(14;16) or t(4;14)]. The primary endpoint was progression-free survival (PFS) in the intention-to-treat (ITT) population. Key secondary endpoints included overall survival (OS). Centralized measurable residual disease by next-generation flow (NGF-MRD) was performed in daratumumab-treated pts. In this analysis we focus on data of the daratumumab-treated cohort.
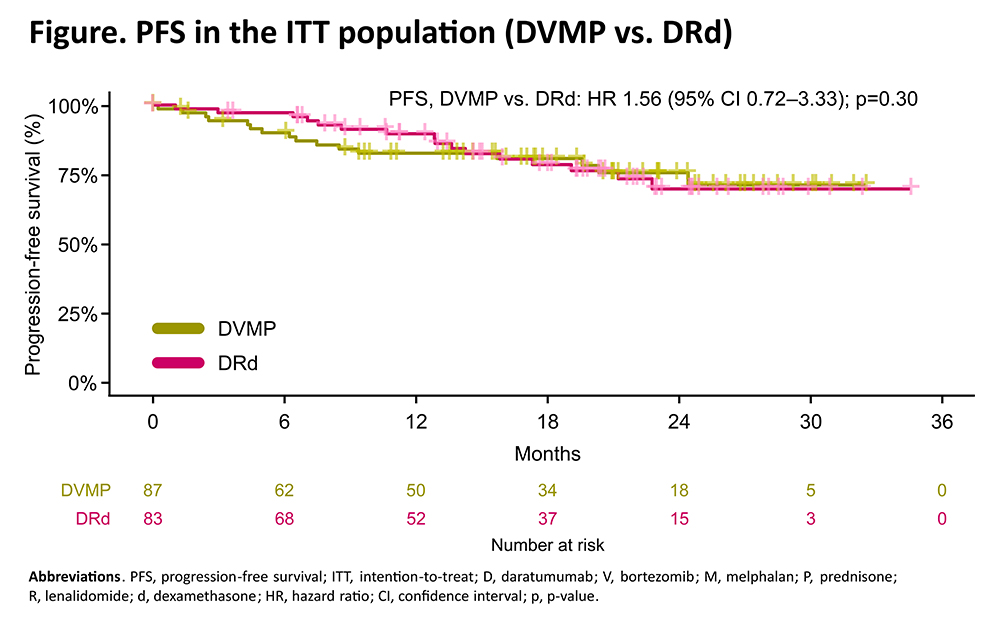
Results. At data cut-off (July 9, 2025), 170 pts received DVMP (n=87) or DRd (83). Baseline characteristics were balanced between DVMP and DRd arms: median age was 76 (range 64–90) vs 76 years (range 63–87); 18% vs 13% of pts were aged >80 years; 37% vs 34% were frail; 27% vs 32% had high-risk cytogenetics. At a median follow-up of 19.3 months, no significant PFS differences were observed between DVMP vs DRd in the ITT population (HR 1.56, 95% CI 0.72–3.33, p=0.30; Figure). No significant differences were observed across age (> or ≤80 years), IMWG frailty score or cytogenetic-defined risk subgroups. The 6-month and 1-year PFS rates were 90% vs 97% and 83% vs 90% with DVMP vs DRd. In the first 6 months, 9 PFS events (2 progressive disease and 7 deaths) were observed [7/9 (78%) pts were frail; 7/9 (78%) events were observed in the DVMP arm]. In the ITT population, the 12-month NGF-MRD negativity rate was 25% with DVMP vs 30% with DRd (OR 1.79, 95% CI 0.81–3.94, p=0.15). Reaching MRD negativity within 12 months led to an improved PFS (vs MRD positivity: HR 0.12, 95% CI 0.03–0.50, p=0.004). No new safety concerns were reported.
Conclusion. We confirmed the efficacy of DVMP and DRd in an older real-life NTE NDMM population including ~35% of frail pts. At current follow-up, no significant PFS differences were observed between DVMP and DRd, but early mortality was more frequent in frail and DVMP-treated pts. Centralized MRD assessment in this real-life setting was feasible, and MRD negativity rates were comparable to those in registrational trials.

Footnotes
Disclosures
No Conflict of interest.
Funding
No funding.
Figures & Tables
Article Information

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.