
Abstract
Introduction. Minimal residual disease (MRD) negativity and sustained MRD negativity are associated with longer survival and are strong prognostic clinical endpoints. PERSEUS (NCT03710603) evaluated subcutaneous Dara + VRd induction/consolidation + DR maintenance vs VRd induction/consolidation + R maintenance in TE NDMM. DVRd significantly improved progression-free survival (PFS), complete response or better rate (≥CR), and MRD negativity rate. Nearly two-thirds of patients on DR maintenance could stop treatment after achieving sustained remission, leading to DVRd being recommended by NCCN as a preferred TE NDMM regimen. Here, we report the impact of sustained MRD negativity status on PFS in PERSEUS.
Methods. TE patients with NDMM age 18–70 years were randomized 1:1 to DVRd (DVRd induction/consolidation + DR maintenance) or VRd (VRd induction/consolidation + R maintenance). The primary endpoint was PFS; MRD negativity rate (MRD negativity 10-5 and ≥CR) was a key secondary endpoint. Sustained MRD negativity, assessed in the intent-to-treat population, was defined as confirmed MRD negativity ≥12 months apart and without MRD positivity in between. Functionally high risk (FHR) was defined as disease progression ≤18 months from treatment initiation, excluding pre-progression deaths.
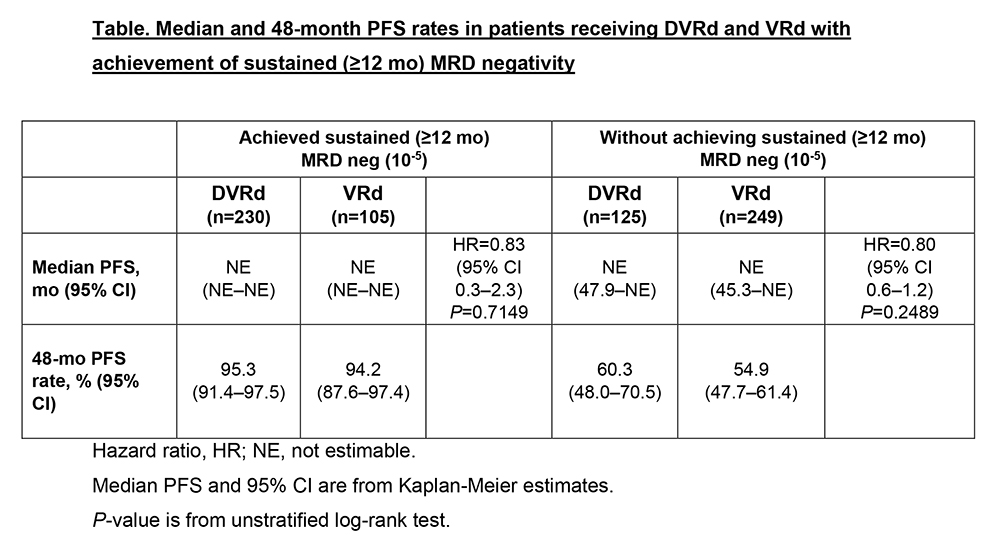
Results. A total of 709 patients were assigned to DVRd (n=355) or VRd (n=354). At 47.5-month median follow-up, ≥12-month sustained MRD negativity rates were higher overall with DVRd (64.8%; n=230) vs VRd (29.7%; n=105); this pattern persisted across clinically relevant subgroups, including age ≥65 years and high-risk cytogenetics. Similarly, ≥24-month sustained MRD negativity rates were higher with DVRd (55.8%; n=198) vs VRd (22.6%; n=80). Patients with ≥12-month sustained MRD negativity vs those without had improved 48-month PFS rates regardless of treatment arm (Table). Compared with VRd, DVRd reduced FHR rates (3.1% vs 6.8%), and rates of FHR or pre-progression deaths were lower with DVRd vs VRd (5.4% vs 11.0%) in the first 18 months.
Conclusions. In TE NDMM, nearly two-thirds of patients treated with DVRd induction/consolidation and DR maintenance achieved ≥12-month sustained MRD negativity, associated with >95% 48-mo PFS rate. Moreover, ≥24-month sustained MRD negativity rates with DVRd were 2.5 times as high as VRd, and FHR incidence was halved with DVRd vs VRd. Collectively, these data further support the PERSEUS regimen as standard of care for TE NDMM. © 2025 American Society of Clinical Oncology, Inc. Reused with permission. This abstract was accepted and previously presented at the 2025 ASCO Annual Meeting. All rights reserved.

Footnotes
Disclosures
No Conflict of interest.
Funding
No funding.
Figures & Tables
Article Information

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.